Craniosynostosis
General Information, Symptoms and Treatment
What is craniosynostosis?
Craniosynostosis is the name given to skull growth and shape problems that occur when one or more skull sutures close too early. This condition is not very rare; approximately 1 case is seen in every 5,000 births. It affects boys slightly more often than girls. It is usually noticeable at birth and becomes more apparent in the following months.
Children with craniosynostosis may have the following findings:
- Bulging at the front or back of the head
- A pointed protrusion in the forehead area
- Depressed temples
- Absence of the fontanelle
- Eyes or eyebrows are not aligned
- A palpable hard ridge along a suture line raised above the skull surface

Neonatal head anatomy
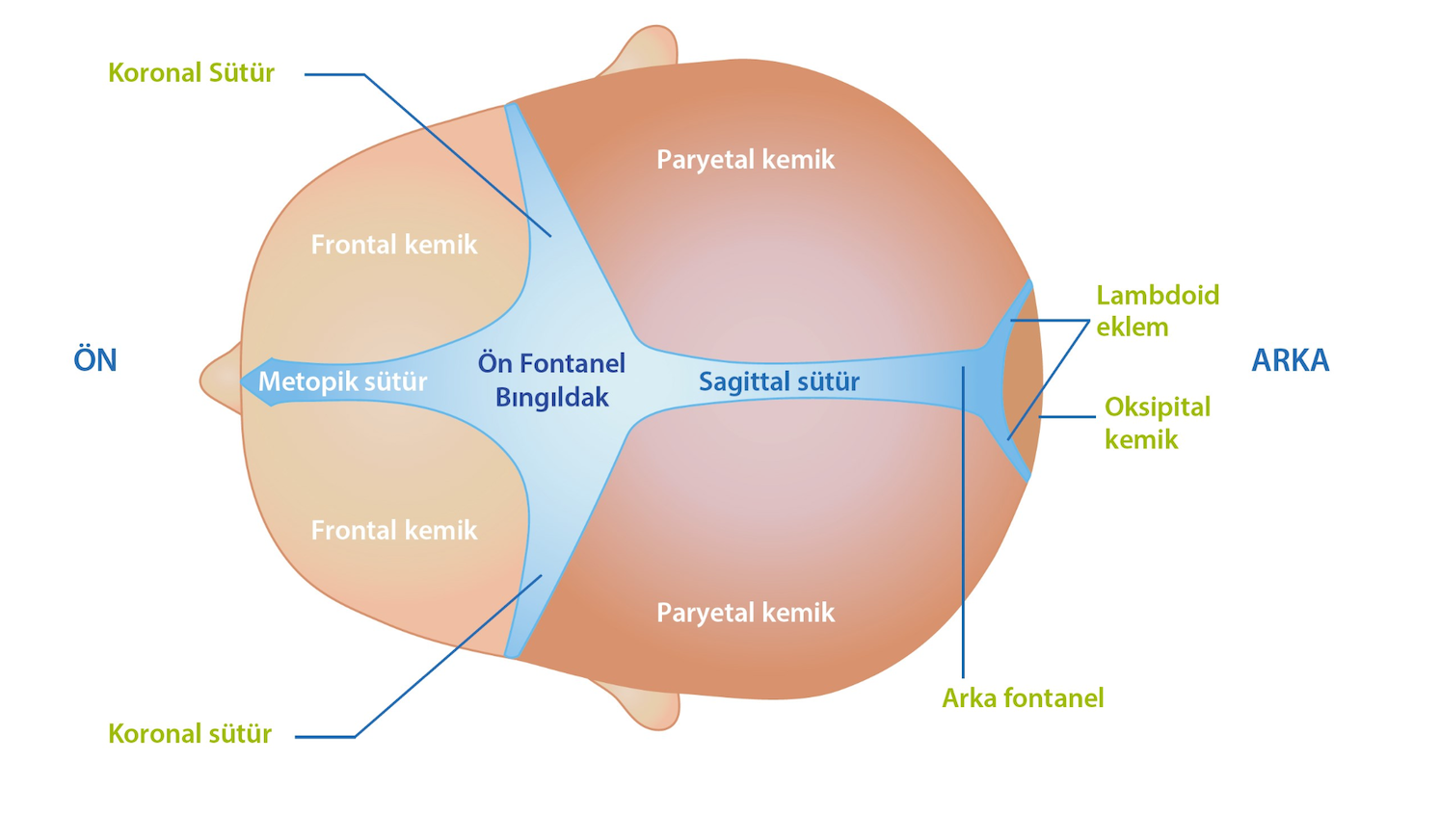
To understand craniosynostosis in a newborn baby, it is helpful to know the anatomy of the skull. The skull is not a single bone. It takes shape when many different bones are connected to each other by joints called sutures. The spaces between these joints are called fontanelles, commonly known as the baby's soft spots. A top view of a baby's skull is shown below.
The sutures are open when a baby is born. These openings allow the skull to grow over time. As the child grows, these joints close and the skull takes its adult shape. Each joint needs a certain amount of time before it closes. For example, the posterior fontanelle may close within 1-2 months after birth, while the anterior fontanelle may close around 18-24 months. Sutures usually remain active until the child reaches adulthood and allow the skull to grow together with the brain tissue inside.
Why does craniosynostosis occur?
The most important thing to know is that nothing you did caused this disease.
Medicines used during pregnancy, foods or drinks, or an accident you experienced are not known to be related to this disease. In most cases, the exact cause is unknown. In some types, called syndromic craniosynostosis, known genetic disorders are thought to play a role.
Types of craniosynostosis
There are many different types of craniosynostosis. They are named according to the affected suture. The most common types are shown in the graphic, and the dashed lines represent the affected suture.

Scaphocephaly (sagittal synostosis): This is the most common type. The front-to-back diameter of the skull is increased. It occurs when the sagittal suture in the middle of the skull closes early.
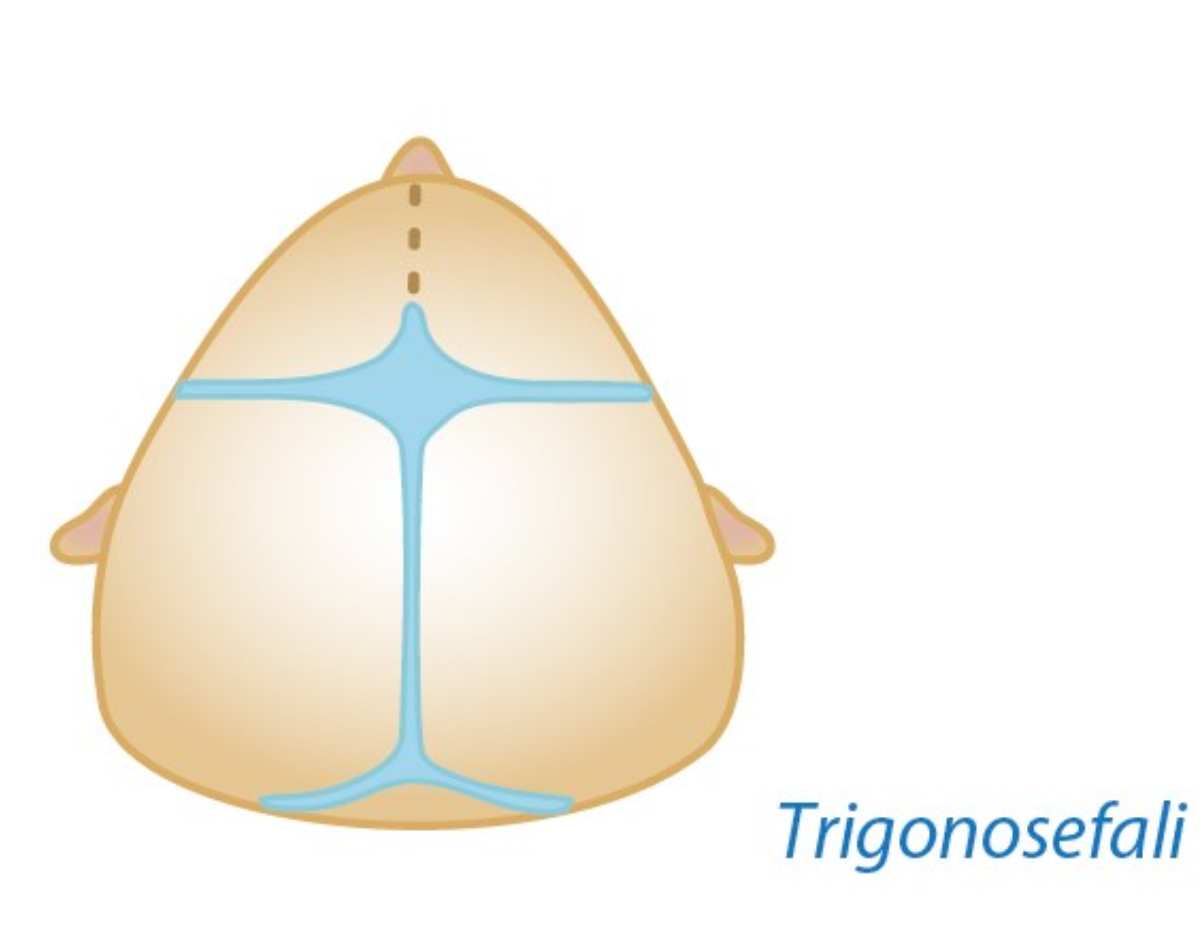
Trigonocephaly (metopic synostosis): This occurs when the suture in the forehead closes early. It causes the skull to point forward, like the bow of a ship. The eyes may appear closer together, creating a false appearance of strabismus.
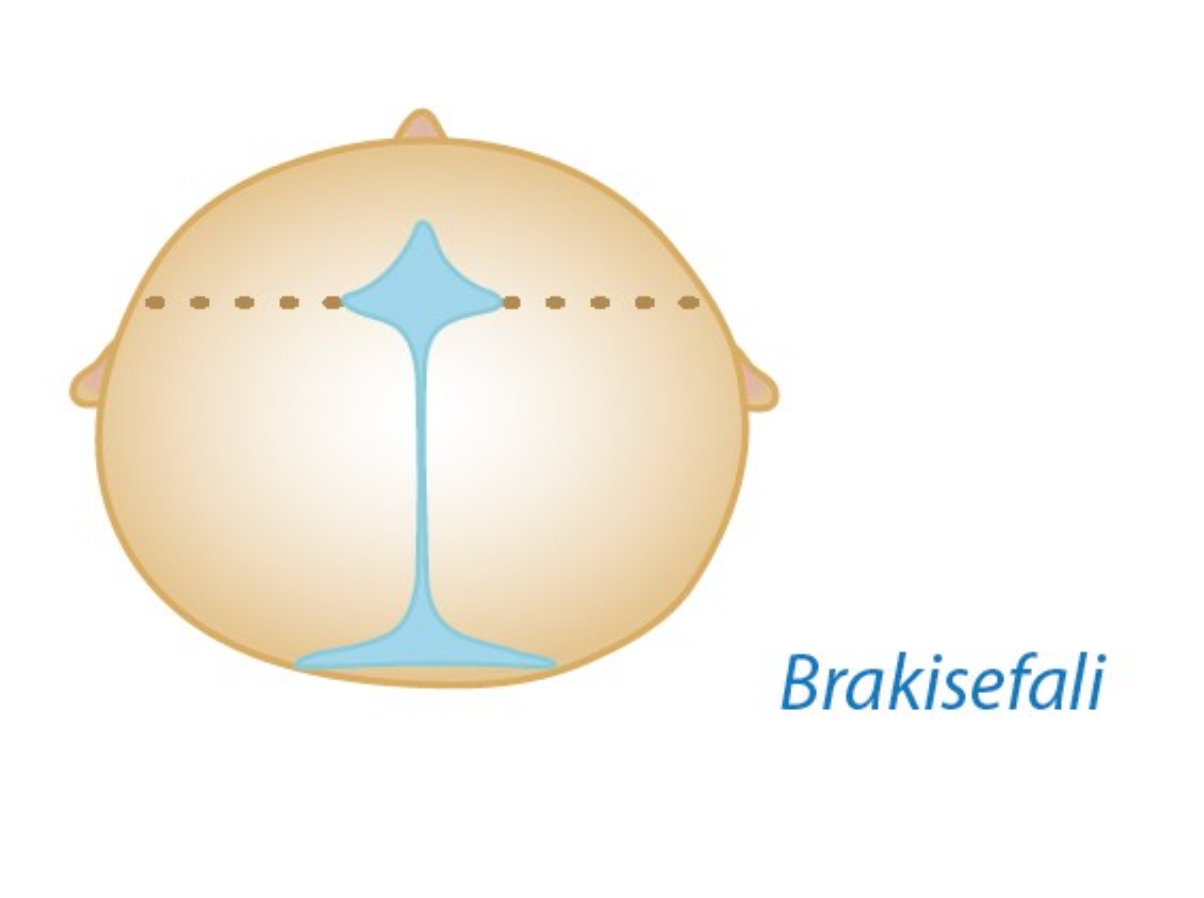
Brachycephaly (bicoronal synostosis): It is caused by closure of both coronal sutures. The head becomes taller upward and the forehead appears flattened.
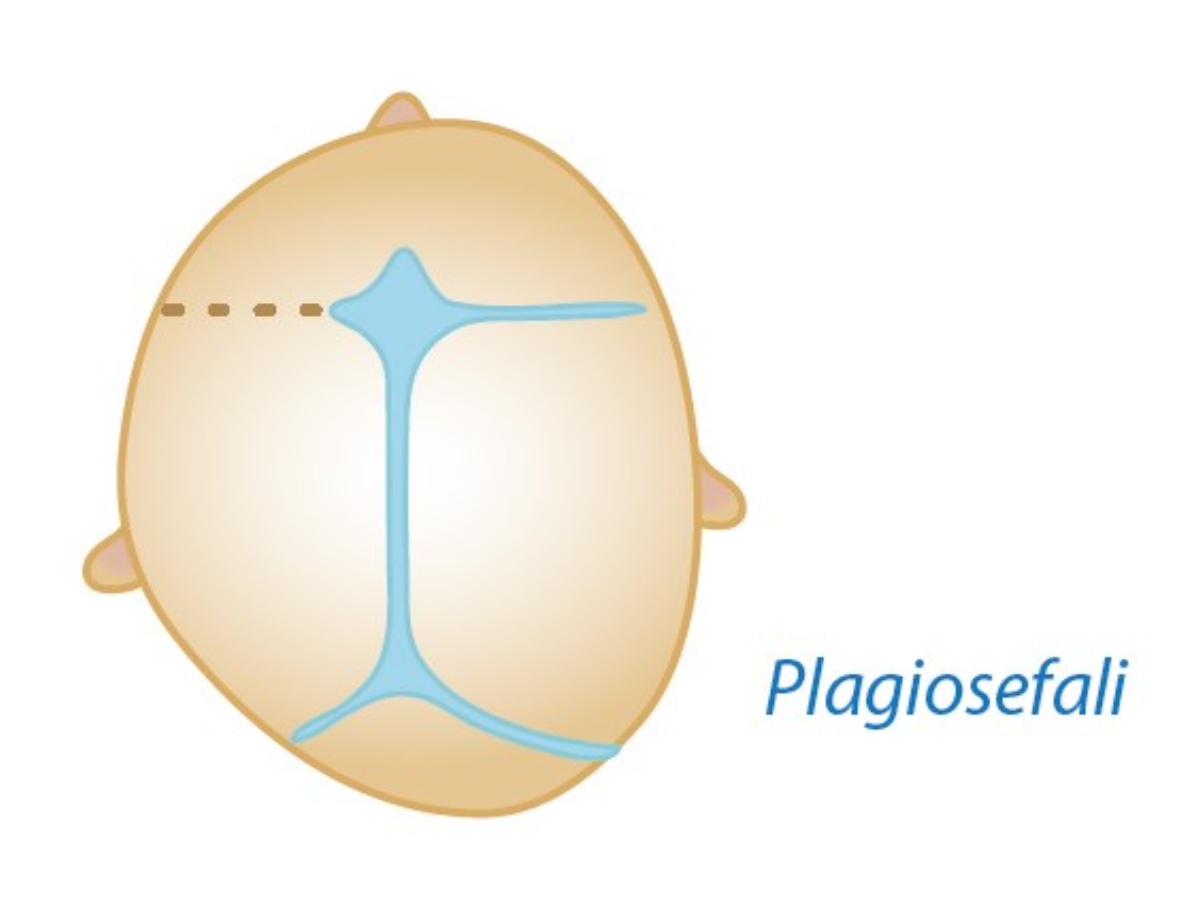
Plagiocephaly (unicoronal synostosis): This forms when a single coronal suture closes. It is one of the more problematic types cosmetically, causing deformity on one side of the head and sometimes downward displacement of the eye on the affected side.
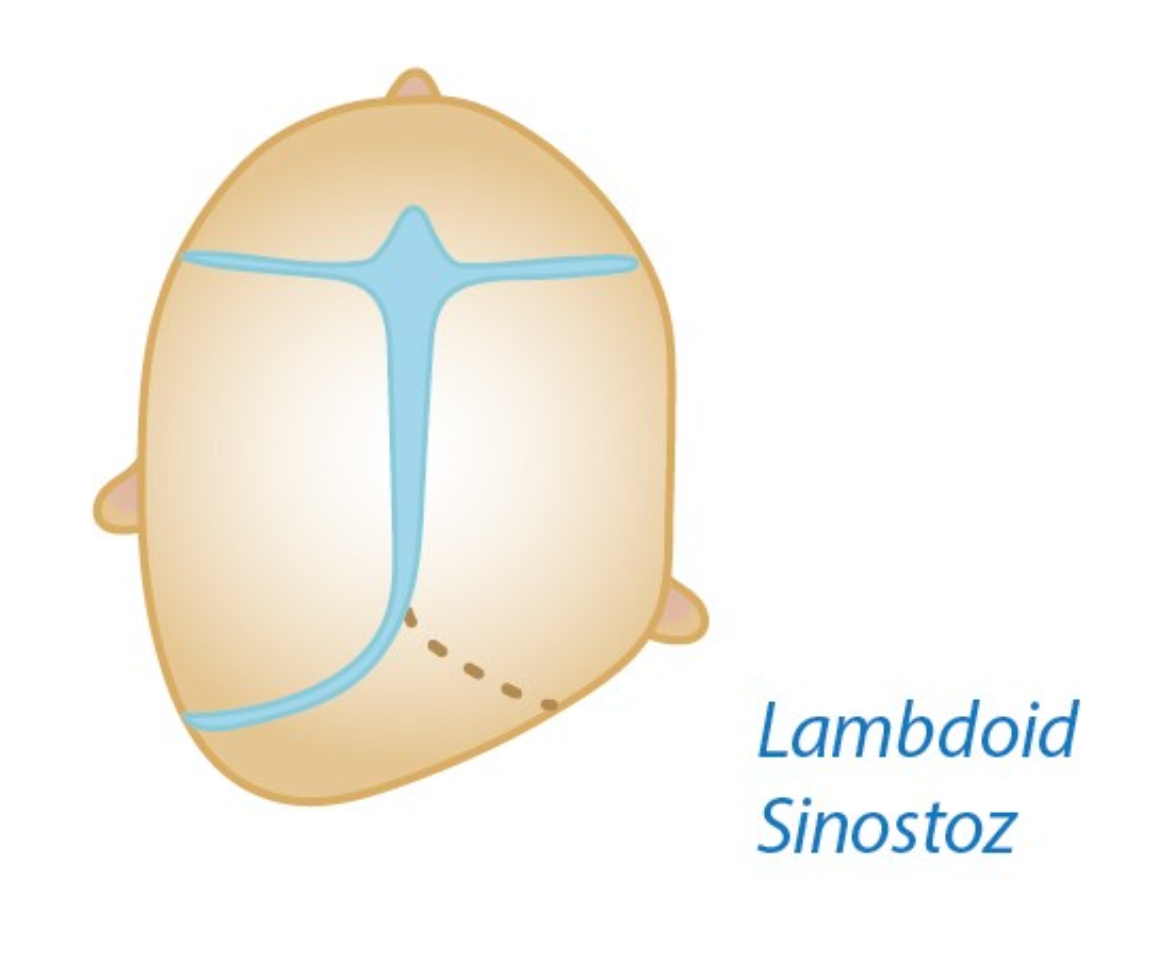
Lambdoid synostosis (posterior plagiocephaly): This is extremely rare. It forms when the lambdoid suture at the back of the head closes. Because it remains under the hair, it may not cause a serious cosmetic finding.
What are the signs of craniosynostosis?
The most obvious finding of craniosynostosis is deformity of the skull. This is usually an aesthetic or visible problem. The severity varies depending on the type of disease. Some patients have problems only in the skull vault, while others also have problems in the skull base, which may appear as asymmetry of the face and eyes. These types are more difficult to treat and may require more than one surgical procedure.
Apart from this main finding, more serious findings may also occur. The most important is increased intracranial pressure, which may develop because skull sutures close too early.
Increased intracranial pressure is more common in syndromic types, where more than one suture is affected. Rarely, it can also be seen with single-suture closure. This pressure increase can appear in different ways. Some possible findings are:
- Persistent headaches
- Eye and vision problems
- Hearing problems
- Developmental delay
- Delay in speech
- Delay in walking
Is surgery necessary in craniosynostosis?
Whether a patient needs surgery is determined by evaluating many different factors. In our clinic, the decision for surgery is made together with the family. The main purpose of surgery is to correct cosmetic, externally visible problems as much as possible.
Children may unconsciously expose a child with a misshapen head to peer bullying. A child with a visibly abnormal head shape may later dislike their appearance and experience psychological difficulties. One of the most important aims is to prevent these problems.
The next important goal is to prevent increased intracranial pressure and related problems, even though the risk is low. Scientific studies suggest that even simple types of synostosis may cause pressure-related problems, but these studies do not provide definitive answers. This remains one of the most debated topics in pediatric neurosurgery.
An image of a scaphocephaly patient sourced from the internet
What are the types of surgical interventions in craniosynostosis?
As in many areas of neurosurgery, unfortunately there is no guaranteed, definitive method. Doctors usually offer options based on available resources, the patient's condition, and their own training and experience. Each surgical method has advantages and disadvantages. The best option will be decided together with your doctor.
Endoscopic Surgery (Closed Surgery): This type of surgery cannot be used for every type of synostosis. The best results are obtained in sagittal and metopic synostosis. The most important factor is the patient's age. It is preferably performed around 3 months of age. In older children, expected results may not be achieved, and it is generally not performed after 6 months.
The biggest advantage of this surgery is that the operation is short and the incisions are small. The biggest disadvantage is that helmet use is required afterward. The helmet is both costly, with insurance coverage varying, and somewhat demanding. It needs to be worn for about 23 hours a day for 6 months. Cosmetic improvement is not immediate and, in some types, may take months or even years.
Open Surgery This is the standard surgical method used for many years and can be applied to all types of synostosis. Surgery is preferably performed between 6 and 12 months, but earlier surgery generally gives better results.
The main disadvantages are that a large incision between the ears is required and surgery can take close to 4 hours (sagittal synostosis surgery takes about 2 hours). The main advantage is that no helmet is needed afterward. Cosmetic improvement is visible immediately. As the wounds heal and the tissue swelling resolves, the desired result is largely reached around the 3rd month.

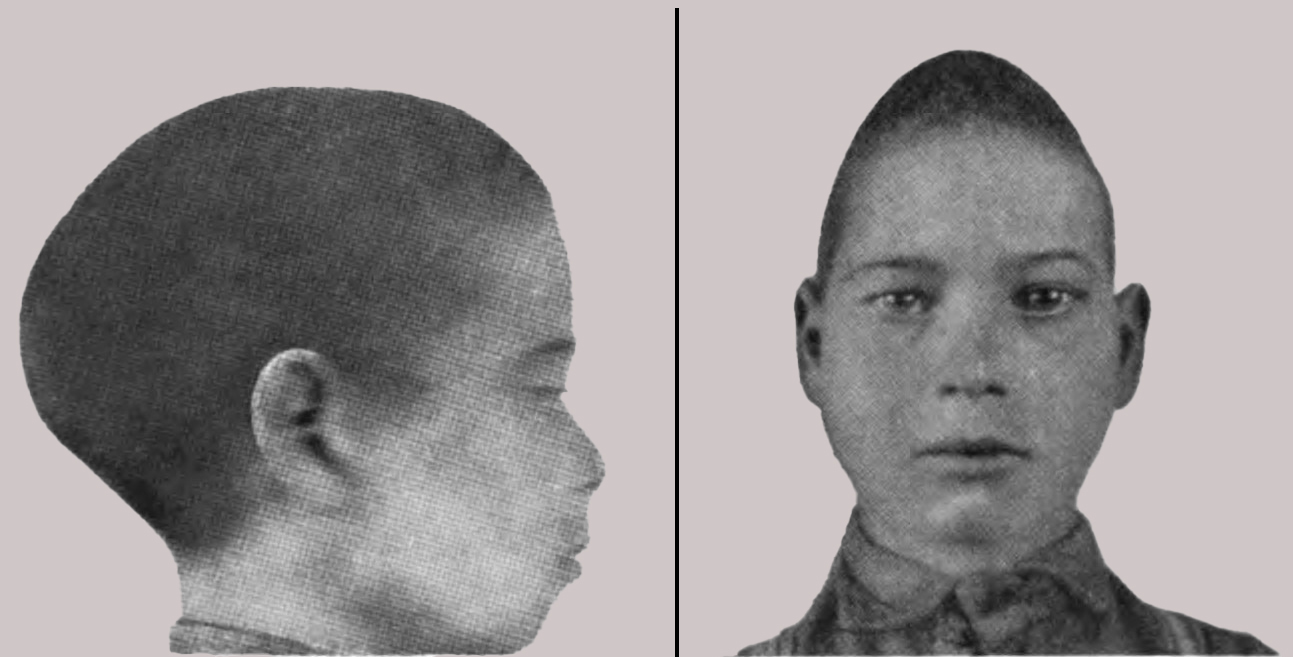
An image of a trigonocephalus patient sourced from the internet
Are there risks of surgical intervention?
Like every surgical and medical intervention, these operations have risks. Craniosynostosis surgery is major surgery performed on a small baby. Operation times are long and blood loss can occur. Therefore, the most important factor that reduces risk is the experience of the team. The surgical team includes neurosurgeons, plastic surgeons, pediatric anesthesiologists and nurses. The anesthesia team has a crucial role in caring for a baby who will remain under anesthesia for a long time. Important details such as body temperature, medical fluid balance and urine output are managed by anesthesiologists. With a good team, surgical risks are kept low.
The most common problems are related to long anesthesia time and blood loss, and are usually managed in the operating room. Other issues such as wound problems, drainage, infection or wound opening may occur. These situations can often be treated as an outpatient, but rarely may require returning to the operating room. Because this is skull surgery rather than brain surgery, problems with brain function are not expected. The most feared life-threatening risk may occur if the problems mentioned above cannot be solved, but the chance of such a serious situation is very low.
Risks of craniosynostosis surgery
The duration of surgery, amount of blood loss and accompanying syndromes determine the level of risk. The risk is lower in healthy babies with a single affected suture; in babies with more than one affected suture or accompanying heart and lung problems, blood and intensive care support may be needed.
- Risk of infection because the incision is short in endoscopic surgery lower, but helmet use is essential.
- Open surgery takes longer; therefore blood transfusion plan is kept ready before surgery.
- In all methods, thanks to an experienced anesthesia team, permanent the risk of neurological damage is very low.
Family blood group compatibility and conditions such as anemia in the baby are addressed before surgery. These preparations reduce overall risk and help prevent unexpected delays.
Recovery process and follow-up schedule
Immediately after surgery, the baby is closely monitored with the family in the intensive care unit until the effects of anesthesia have fully worn off. Babies in stable condition are transferred to the ward the same day, and I allow the first feeding while they are still in intensive care. If there is no special medical reason, they do not need to spend the night in intensive care.
- Discharge: After open surgery, discharge is usually on the 4th day. After endoscopic (closed) surgery, babies can often go home the next day.
- First month: Swelling reduction and stitch absorption are followed. If helmet treatment is needed, measurement and fitting are done during this period.
- 3rd month: Head circumference and cosmetic improvement are evaluated with photos, and neurodevelopmental tests are planned.
- 1. year: Skull growth is checked with imaging, and helmet treatment, if used, is completed.
In the long term, head shape and neurodevelopment are followed with regular check-ups. Most children continue their activities smoothly in the preschool period.
Family experiences and sources of support
Talking with families who have gone through the same process can reduce the emotional burden before and after surgery. Parents in Turkey in the "Craniosynostosis Families" communities on Facebook share their daily experiences and practical advice about surgery, helmet fitting and follow-up visits.
Taking notes from online posts and sharing what you have heard with your doctor at follow-up visits helps balance online information with reliable medical advice.
Frequently Asked Questions
After surgery, a large turban-style dressing will be wrapped around your child's head. This dressing starts from the lower part of the head, passes over the ears and extends to the forehead. The head of your child's bed will be elevated 30 degrees and kept that way until discharge. This supports drainage from the surgical site and helps reduce swelling.
A significant amount of fluid will build up around the face and eyes. You may hear this called edema. Edema is a very normal response to a procedure such as surgery. Your child will most likely have some swelling after surgery; this is expected. Most children have swelling, and if reshaping was done in the front of the head, they may not be able to open their eyes at first. Swelling peaks around the second day after surgery and then gradually decreases. By discharge, the eyes are usually open. Bruising related to swelling also decreases during the first postoperative week.
Your child will be taken to the intensive care unit after surgery. This is usually a precaution, not because their condition is poor. In intensive care, the team waits until the child is fully awake and able to suck or feed, and the child is transferred to the ward as soon as the doctors consider it appropriate. Sometimes an overnight stay in intensive care may be needed, but usually the child is taken to the room on the day of surgery. Your doctor will inform you at every stage, so there is no need to worry.
Hospital stay usually depends on reduction of facial swelling, feeding after surgery and resolution of the fever that is often seen after operations with a large wound. Discharge is usually on the 4th or 5th day.
The reshaping procedure is usually well tolerated by most children with minimal discomfort. Older children who have this procedure often do not complain of significant pain. However, each child has a different pain threshold, and pain-relieving medicines are available for any postoperative pain.