Brain Tumors
Frequently Asked Questions
Prof. Dr. Alp Özgün Börcek at Ankara Güven Hospital provides pediatric and adult neurosurgical evaluation for brain tumors, including treatment options such as surgery and Gamma Knife radiosurgery. The content below is general educational information; diagnosis and treatment planning require individual clinical assessment.
The answers below reflect current medical knowledge and address common patient questions about brain tumors and surgery. Each case should be evaluated individually, and final treatment decisions should be made together with your treating physician.
What are the symptoms of a brain tumor?
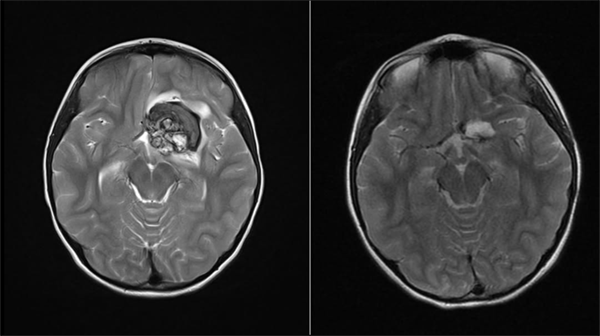
Brain tumors may cause symptoms such as headache, nausea, vomiting, balance problems, and changes in vision or speech. Symptoms can vary depending on the location of the tumor.
What is a brain tumor?
A brain tumor is a mass formed by the uncontrolled growth of cells in or around the brain. Brain tumors may be benign or malignant.
What causes a brain tumor?
Most brain tumors are random, but genetic factors, radiation exposure and prolonged contact with certain chemicals may increase the risk.
How is brain tumor surgery performed?
In brain tumor surgery, advanced techniques such as the surgical microscope and neuro-navigation are used to remove the tumor as safely as possible. The goal is to remove as much of the tumor as safely as possible while preserving brain function.
The answer depends on the patient's condition at the time of
admission, symptoms, neurological examination findings, MRI
and other imaging findings, the preferences of the child's
legal guardian, and most importantly the doctor's
recommendation. Because Neurosurgery deals with very delicate
tissue and carries somewhat higher risks than many other
fields, follow-up is always one of the options considered.
If the patient is not being affected by the problem and the
criteria above are suitable, your doctor may decide to follow
the patient and monitor how the condition changes over time.
For example, new imaging may be requested after 3 to 6 months
and the situation can then be reassessed.
On the other hand, if the patient is affected by the disease
(for example, having epileptic seizures, vision problems, or
weakness in an arm or leg), or if the imaging suggests that
follow-up would be risky, your doctor may recommend surgery.
Each patient is evaluated individually, and in medicine no
two patients are exactly alike. A neighbor's child with a
similar problem may not need surgery, while surgery may be
recommended for your child. Or a change seen on follow-up
imaging may lead to a decision for surgery.
The decisions made by the doctor you trust are individual
decisions made for the benefit of you and your child.
With advances in technology, radiological imaging gives us much more information than it did 10-15 years ago. In many diseases, imaging provides very important clues and helps your doctor form an opinion about the condition. However, no method other than examining tissue can yet provide a definite diagnosis. Therefore, in patients who need surgical intervention, removing part of the pathological tissue (biopsy) or removing it completely is essential. The tissue is examined under a microscope, the diagnosis is learned, and the next steps in treatment are decided accordingly.
Personally, in non-emergency situations, I encourage my patients to seek opinions from other doctors as well. The most important point to remember is that medicine is not always as simple as two plus two equals four. We are dealing with the human body, and nervous system tissue is one of the body's most delicate tissues. Each doctor will give an opinion based on their own knowledge and experience. One doctor may recommend surgery while another may suggest waiting a little longer, or one doctor may recommend one type of surgery while another recommends a different operation, and both may be medically reasonable. What matters is the decision you make and the trust you have in the doctor who will guide treatment. Trust in your doctor is an important factor in the course of care.
The most important principle of Neurosurgery, as in other fields, is first to avoid harming the patient and, whenever possible, to help the patient come out of surgery without new problems. For this reason, the accepted scientific approach is to remove the tumor in the safest possible way. Technically, many lesions in the brain can be removed, but what matters most is the patient's condition after the procedure. If the entire tumor is removed but the patient can no longer walk or see, it is difficult to call that a successful treatment. Brain tissue is very delicate, and once it is damaged, lost functions may not always return. For this reason, neurosurgeons take great care to preserve the patient's walking, speech, vision, and overall neurological condition after surgery. Your doctor may therefore avoid surgical steps that could harm the patient and, if necessary, may not remove the entire tumor. For example, when a tumor involves vital brain structures, the parts that can be safely removed may be taken out while risky areas are left behind. This decision is often guided by preoperative imaging, but the final decision is usually made during surgery, when the surgeon is directly facing the brain tissue and the tumor. Unfortunately, even when every precaution is taken, some patients may lose certain functions after surgery. This is related to the sensitivity of the organ treated in Neurosurgery. In some cases, if the risk to life is high, possible functional losses may be weighed differently and the tumor may be removed more aggressively. Your doctor will explain all of this together with the preoperative and postoperative test results.
As you know and as almost every doctor explains, every surgical intervention carries risks. This is true for the simplest operations as well as the largest ones. Risks may range from simple drug allergies and wound problems to, very rarely, coma or death. In Neurosurgery, there are also risks that can affect quality of life, such as arm or leg weakness, facial paralysis, vision loss, or prolonged difficulty waking up. Your doctor will explain these risks before surgery. Every operation is serious, and every precaution is taken to prevent problems. Still, the human body is not like a machine, and its reactions cannot always be predicted. Risks can occur despite all precautions. Fortunately, complications such as death and coma are very rare. Other complications may be temporary and improve over time.
Because brain tissue is very sensitive, neurosurgeons do not want anything inside the skull that could disturb it. For this reason, rarely, problems such as bleeding seen on the first imaging after surgery may require a second operation. Your doctor will give you detailed information about this.
If a tumor cannot be completely removed during surgery, this does not mean that the disease is untreatable. Neurosurgery works closely with radiation oncology and medical oncology. Depending on the tumor type, radiation treatment and medication may be considered after surgical treatment.
Cancer surgery, or oncologic surgery, is a field in which very challenging diseases are managed and treated. As in other branches, treatment options in Neurosurgery vary greatly according to the type of pathology. Brain tumors are usually classified by grade. A grade 1 tumor is considered the most benign, while a grade 4 tumor is considered the most malignant. In benign brain tumors, complete removal often reduces the need for additional treatment. In malignant tumors, however, even when the entire tumor is removed, current medical knowledge and evidence often support additional treatments. The main purpose is to reduce the chance of the tumor recurring. Another important point is not only the tumor type but also its location in the brain. For example, even a benign tumor on the optic nerve or in the brainstem, a vital area, may carry as much or even more risk than a malignant tumor in a different brain region. Treatment decisions are made by considering all these features, and the most appropriate option for your child is chosen.
Brain tumors differ from tumors in other organs in many ways. Even a benign tumor that has been completely removed can, rarely, recur after a long time. Although this possibility is very low, I recommend lifelong follow-up with a neurosurgeon. Follow-up visits are more frequent in the first years and are gradually spaced out to once a year, and later to every two or three years.
In general, the answer is no. Of course, larger problems may take longer to solve, but families should know that the surgeon is not operating during the entire time the patient spends in the operating room. Preparation before anesthesia and the time needed to wake the patient after surgery also affect the total operating room time. Preparation before surgery in a young child can sometimes take more than an hour. Doctors make every effort to keep anesthesia time as short and safe as possible.
No. In Neurosurgery, the pathways used to reach the nervous system and perform the necessary operation have been defined for many years and usually do not change according to the severity of the disease. The size of the skin incision is planned to allow the surgeon to perform the operation in the safest way. The number of skin stitches at the end of surgery depends largely on the surgeon's habits. Sometimes dozens of stitches are used, while in suitable patients internal stitches that are not visible from the outside may be used. The number of stitches is not a measure of the size or seriousness of the operation.
After brain surgery, cerebrospinal fluid leakage from the
wound can sometimes be seen. Even when the skull is closed
carefully, this type of complication may occur. If this
happens while your child is still in the hospital, your
doctor will take the necessary precautions. These measures
may include returning to the operating room to find and
repair the leak.
If you notice this problem after discharge, please contact
your doctor as soon as possible.
Your doctor will explain everything you need to know. Unless
you are told to pay attention to something specific, I
generally do not place major restrictions on my patients
after brain surgery.
Returning to school as soon as it is medically appropriate
can help children move away from the psychology of illness.
You will be given advice about eating and drinking, how to
use medications, and when to come for follow-up visits.
In our clinic, when appropriate, the skull is closed with plates and screws after it has been opened, and these systems provide a very strong closure. If your child bumps their head soon after surgery, there will most likely not be a serious problem. Still, for any situation that worries you, contact your doctor. If you cannot reach your doctor, it is best to seek an opinion from a nearby neurosurgeon.