Lumbar Disc Herniation
General Information, Symptoms and Treatment
Prof. Dr. Alp Özgün Börcek provides diagnosis and treatment for lumbar disc herniation at Ankara Güven Hospital within pediatric and adult neurosurgery and spine surgery. The information on this page is general; an examination is required for personal assessment.
THE FOLLOWING IS GENERAL INFORMATION ABOUT LUMBAR DISC HERNIATIONS AND MAY NOT APPLY IDENTICALLY TO EVERY PATIENT.
LOW BACK PAIN CAN HAVE MANY CAUSES OTHER THAN HERNIA AND THESE SHOULD BE INVESTIGATED.
FOR THE MOST ACCURATE DIAGNOSIS AND TREATMENT PLAN, PLEASE CONSULT A NEUROSURGERY SPECIALIST.
Which Department to Go to for Low Back Pain?
Patients with low back pain may initially consult either Neurosurgery or Physical Therapy and Rehabilitation . In clinical practice, surgical treatment of lumbar disc herniation is typically performed by neurosurgeons, while physical therapy teams focus on conservative care such as exercise programs, rehabilitation, and non-operative pain management. The most appropriate specialty depends on symptom severity, duration, and neurological findings.
Which doctor should I see for low back pain?
Low back pain is often caused by muscle strain, postural overload, or age-related disc degeneration. Many causes are treatable with conservative care, and early referral to the right specialty can shorten recovery time.
- - Mild (< 6 weeks, non-traumatized) - Primary Care / Physical Therapy and Rehabilitation
- - Numbness / weakness in the leg - Neurosurgery
- - Fever, night pain, weight loss - Physical Therapy and Rehabilitation Infectious Diseases / Oncology
- - Pain associated with pregnancy - Gynecology → Physical Therapy and Rehabilitation
- - Serious trauma (fall, accident) - Emergency Department → Orthopedics
In many cases, medication, structured exercise, and lifestyle changes are sufficient. Surgery is needed only in a selected subgroup of patients.
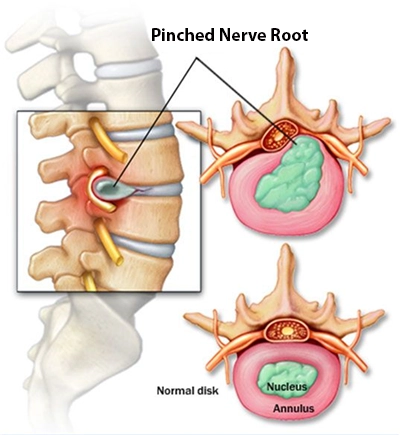
What is lumbar disc herniation? Is there such a thing as a "ruptured disc"?
The human spine is composed of vertebrae separated by intervertebral discs, which function as shock absorbers. Each disc has a softer inner core and a firmer outer ring. With aging, repetitive loading, or trauma, disc material can protrude and irritate adjacent nerve roots. This condition is called lumbar disc herniation.
Common questions about "disc rupture" are answered in the FAQ section below.

Why does our lower back hurt?
LOW BACK PAIN IS ONE OF THE MOST COMMON REASONS FOR SEEKING MEDICAL CARE.
A major reason is natural age-related change in spinal tissues over time.
LOW BACK PAIN DOES NOT ALWAYS MEAN A DISC HERNIATION OR A SURGICAL PROBLEM.
Clinical evaluation focuses on pain pattern, duration, neurological findings, and response to rest, exercise, and medical treatment.
Pain can be severe even when the underlying pathology is non-surgical. Many episodes improve with conservative treatment, and only a minority require surgery.
What are the Symptoms of Lumbar Disc Herniation?
Lumbar disc herniation may present with low back pain that starts suddenly or gradually. Pain can radiate to the leg and may be accompanied by numbness, tingling, or weakness. Symptoms often worsen with coughing, sneezing, prolonged sitting, or straining. Early specialist evaluation is important when neurological symptoms are present.
When should you consult a doctor for back pain?
If your pain is persistent, severe, or worrying, you should seek medical assessment. A primary care physician, physical medicine specialist, or neurosurgeon can guide the next step.
Beware of Red Flags!
Red flags include new weakness in the foot or leg, urinary retention, or urinary/fecal incontinence.
Seek urgent review if pain is progressively worsening despite treatment or wakes you from sleep at night.
If your back pain started after a fall or accident,
Fever accompanying back pain requires prompt assessment.
If you have a history of cancer, unexplained weight loss, or new persistent back pain, urgent evaluation is recommended.
Long-term high-dose steroid use with new back pain is another warning sign.
YOU SHOULD DEFINITELY CONSULT A SPECIALIST DOCTOR.
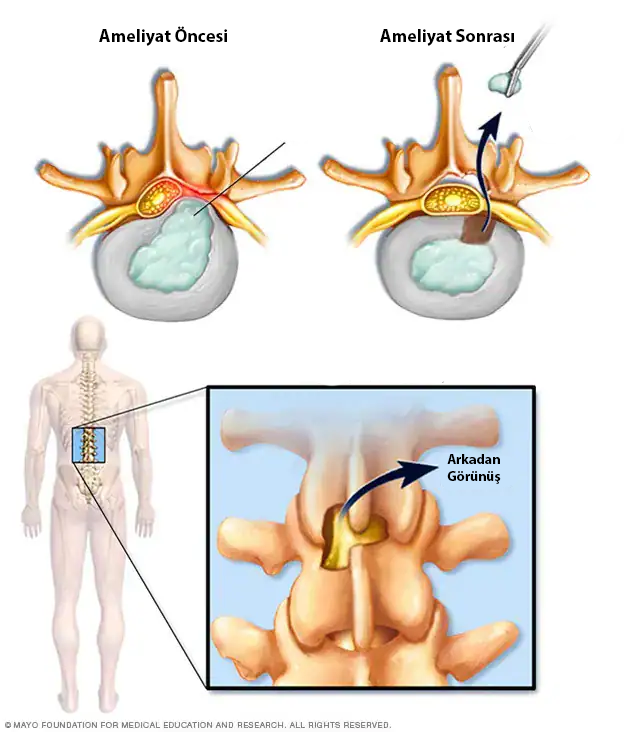
How is Lumbar Disc Herniation Treated?
Treatment is individualized according to symptom severity, neurological status, and imaging findings. First-line care usually includes medication, activity modification, and structured physical therapy. Core strengthening and posture-focused rehabilitation are effective for many patients. In selected cases, injection-based pain procedures or surgery may be needed.
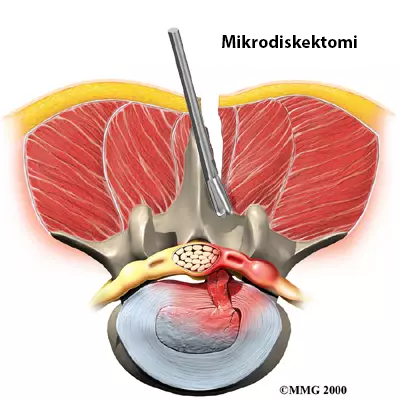
Lumbar Disc Herniation Surgery
Lumbar disc herniation surgeries have been performed successfully for many years and are reliable methods...
Minimally invasive or closed techniques are not suitable for every patient...
Open surgery can be applied to a wider group of patients...

After surgery, patients are helped to stand as soon as possible and are encouraged to return gradually to daily life...
Why Is Lumbar Disc Herniation Surgery Often Feared and Avoided?
Lumbar disc herniation surgery is frequently misunderstood and therefore feared more than it needs to be. People often make decisions based on hearsay or on a negative experience reported by a relative or acquaintance. However, every patient is different and every treatment plan is individualized. One of the most common misconceptions is this: "People think that after back surgery their back will never hurt again; when back pain occurs later, they assume the surgery did not work." However, lumbar disc herniation surgery aims only to remove the disc tissue pressing on the nerve. It does not completely reverse worn discs or years of degenerative change. For this reason, occasional low back pain can be part of the natural process and does not mean the surgery has failed. Making decisions from individual stories rather than reliable medical information can delay treatment and create unnecessary anxiety.
Frequently Asked Questions
This is one of the most common misconceptions among the general public. The likelihood of becoming wheelchair-bound because of a lumbar disc herniation or lumbar disc surgery is extremely low. However, "cauda equina syndrome" and "conus medullaris syndrome", two very rare conditions special conditions may increase this risk. These syndromes are usually associated with large disc herniations and may require emergency surgery. If left untreated, paralysis risk may arise. Fortunately, such situations usually cause clear symptoms that lead the patient to seek medical care.
Apart from these exceptions, complete paralysis due to lumbar disc herniation is almost impossible. The nerves leaving the lumbar spine send signals to specific muscle groups in the legs. A disc herniation usually affects one nerve, so weakness or loss of movement is usually limited to the muscle group controlled by that nerve. For example, a disc herniation between L4-L5 can affect the nerve that lifts the foot upward, causing "foot drop." This condition usually requires urgent treatment, and recovery after surgery is often good.
The phrase "ruptured disc" is sometimes used to explain the situation more clearly to patients, but it is not a precise medical definition. A disc herniation does not literally burst or leak in the way the phrase suggests. Over time, larger disc herniations may allow inner disc material to move outside the disc. This can mean that the herniation has progressed and that pressure on the nerve has increased. However, it does not always mean that surgery is necessary. Only your doctor can decide whether surgery is needed.
The condition described to you as a "ruptured disc" is probably a larger-volume lumbar disc herniation. However, the treatment approach for large herniations is based on the same principles as for smaller ones. The word "ruptured" does not by itself mean the condition is worse or unsolvable. What matters is the clinical picture caused by the disc herniation.
As mentioned earlier, it is extremely unlikely for a lumbar disc herniation to cause paralysis. In disc herniations that require surgery, the main problem is usually pain that seriously affects quality of life and makes daily activities difficult.
Contrary to common belief, not every lumbar disc herniation requires surgery. Many disc herniations can be controlled with medication, physical therapy and lifestyle changes.
What matters is whether the disc herniation responds to treatment and whether it causes weakness in a leg muscle group. Even when muscle strength is reduced, surgery is not mandatory in every case. This decision should be made by the doctor who listens to you and examines you.
The answer involves many genetic and environmental factors and is a broad topic. The most basic reason, however, is increasing structural wear in the spine over time. Just as our skin wrinkles or our hair turns white with age, the spine also wears through natural processes.
After flu-like illnesses, low back pain is one of the most common reasons people seek medical care, and almost everyone experiences it at some point. From the moment humans began walking on two legs, the spine has carried constant load against gravity. Over time, this can cause the intervertebral discs to lose flexibility and may contribute to disc herniation.
In addition to natural aging, excess weight, a sedentary lifestyle, heavy lifting and some metabolic diseases can also contribute to lumbar disc herniation.
REMEMBER: Lumbar disc herniation is not the only cause of low back pain. Consulting a specialist for correct diagnosis and appropriate treatment is extremely important.
As mentioned earlier, lumbar disc herniation is often the result of natural wear that develops in the spine with age. Findings described as "herniation" in MRI reports often reflect this aging process on imaging.
Especially from the 20s onward, disc herniation or herniation-like changes may be seen on MRI in many people. However, many of these findings are part of the normal aging process and are often not directly related to the patient's complaints.
Therefore, it is not correct to say "you need surgery" by looking only at the MRI report. What matters is whether the imaging findings match the patient's clinical condition. The person who will evaluate this is your doctor.
PLEASE REMEMBER: We treat patients, not MRI films. Although your report may contain numerous findings, in most cases, surgical treatment may not be needed.
In medicine, every disease and every patient is unique. A treatment that is successful for one person may have different results for another person with the same condition. For this reason, medical decisions often depend on probabilities and rates rather than absolute rules. Lumbar disc herniation is an example of this.
Lumbar disc herniation can recur. There are many discs in the spine, and each has the potential to herniate. During surgery, only the problematic disc level is treated; the others are left untouched. For this reason, disc herniation may occur at other levels in the future.
In addition, the operated disc may herniate again at the same spot. This recurrence rate is generally between 5% and 15%. Recurrent disc herniation may occur soon after the first surgery or years later. However, not every recurrence requires another operation. Your doctor will make the best decision according to the severity of your complaints and your neurological findings. In some cases, a second and rarely a third operation may be needed.
Lumbar disc herniation surgeries are generally safe procedures with a low complication rate. However, as with every surgical intervention, there are some risks.
The most common risks include infection, pain at the incision site, irritation of nerve tissue and, rarely, nerve damage. Much more rarely, bleeding, cerebrospinal fluid (CSF) leakage or recurrent disc herniation may occur.
These risks are minimized when surgery is performed by an experienced neurosurgeon. Most patients recover quickly and smoothly after surgery.
Pain may continue for a while after lumbar disc surgery, and this is usually considered normal. Temporary pain, tingling or numbness may occur while the nerve tissue and surrounding tissues heal.
These symptoms usually decrease over time. However, if your pain is very severe, increasing, or lasting longer than expected, you should consult your doctor. In some cases, persistent severe pain may be a sign of an additional problem or complication.
If you do not have the chance to rest, simple but effective measures in daily life may help reduce the pain. Avoid staying in the same position for long periods; take short breaks and do light stretching whenever you can.
Using an ergonomic chair, using pillows to support your lower back, and applying a warm towel to the low back area may relax the muscles and reduce pain. Regularly practicing simple exercises recommended by your doctor to strengthen the low back and abdominal muscles can also support pain control.
To relieve pain radiating to the leg from a lumbar disc herniation, you can try resting positions that reduce pressure on the nerve. For example, placing a pillow under your knees while lying on your back or lying on your side in a fetal position provides relief for many people.
Gentle stretching exercises for the low back and leg muscles, such as bringing the knees toward the chest or stretching the hamstrings, can reduce tension on the nerve. A warm shower or warm application to the low back may also ease pain by relaxing the muscles.
If your pain is very severe, using a pain reliever recommended by your doctor may also be helpful.
Spa or hot water treatment can help relieve pain related to lumbar disc herniation. Heat relaxes muscles, improves circulation and provides general relaxation. Many people report less low back pain and stiffness after a hot bath or spa.
However, hot treatments are only supportive; they do not remove the disc herniation itself. For this reason, hot water treatment should be used together with exercises and other treatments recommended by your doctor.
Swimming is one of the most commonly recommended activities for people with lumbar disc herniation and can be a very useful exercise. The buoyancy of water reduces the load on the spine, so the low back is not exposed to excessive pressure during movement.
Swimming can also strengthen the back and abdominal muscles, support the low back and contribute to pain reduction. However, it is important to avoid sudden or forceful movements that strain the low back and not to overdo it.
When you have a lumbar disc herniation, demanding activities such as high-tempo running can overload the spine and increase pain. Therefore, you should be careful. Because each person's situation is different, lower-impact exercises such as brisk walking or swimming may be preferred during recovery instead of jogging.
In the gym, heavy lifting or movements that directly strain the spine are generally not recommended. Instead, focus on light strengthening exercises recommended by your physiotherapist. If a movement causes pain, avoid that exercise.
Long car trips or air travel may increase discomfort in people with lumbar disc herniation because of prolonged sitting. However, with care, they usually do not cause permanent damage.
Inactivity increases pressure on the spine and can cause muscle stiffness, triggering pain. To prevent this, it is helpful to take regular breaks, walk when possible, or stand and move during a flight if conditions allow.
Using a small lumbar support pillow while sitting and changing position frequently also helps reduce the load on your low back.
Mattress choice is important in lumbar disc herniation. In general, medium-firm or firm mattresses are preferred over very soft ones. A supportive mattress may help keep the spine in a more natural position during the night and reduce the load on the low back.
Many people report that very soft beds increase low back pain, while medium-firm or firm mattresses allow more comfortable sleep. However, "firm mattress" does not mean a hard surface like wood; it means a mattress that supports the body without collapsing.
The ideal mattress is a medium-firm orthopedic mattress that supports the body's natural curves and preserves the lumbar curve.
Lumbar disc herniation pain is mainly caused by a physical problem; these pains are real, not imaginary. However, stress, anxiety and similar emotional factors can significantly influence pain perception.
Under intense stress, the body's sensitivity to pain increases and muscle tension may develop. This can trigger existing low back pain or make it feel more severe. In other words, the same physical problem may cause more discomfort during a stressful period.
For this reason, relaxation techniques, stress management and a regular sleep routine can support coping with low back pain.